








{kind=link}
E. Amory Codman Pioneer New England Shoulder Surgeon
by Bill Mallon, M.D.
E. Amory Codman was a New England based shoulder surgeon, born just after Rutgers defeated Princeton in the first college football game (1869); and who died as the  Luftwaffe was strafing London (1940). In his youth, anaesthesia was made viable to ease the suffering of surgery. At the dawn of his surgical career, Wilhelm Röntgen discovered x-rays, and Codman died as the antibiotic era became reality. He is known for many things, shoulder surgery among them, but for his work in promulgating the need to do outcome studies, he should be considered one of the most important surgeons of the 20th century. But sadly, that has not occurred.
Luftwaffe was strafing London (1940). In his youth, anaesthesia was made viable to ease the suffering of surgery. At the dawn of his surgical career, Wilhelm Röntgen discovered x-rays, and Codman died as the antibiotic era became reality. He is known for many things, shoulder surgery among them, but for his work in promulgating the need to do outcome studies, he should be considered one of the most important surgeons of the 20th century. But sadly, that has not occurred.
Codman was born in Boston, of a Boston Brahmin family. He attended The Fay School in Southborough, and later went to high school at the St. Mark’s School, also in Southborough. Codman then attended Harvard College, and later graduated from Harvard Medical School in 1895. He then joined the staff at Harvard, practicing as a general surgeon at Mass General.
Ernest Amory Codman was a pioneer in six different fields of medicine – anaesthesiology, radiology, duodenal ulcer surgery, orthopaedic oncology, shoulder surgery, and the study of medical outcomes. Had his life been less troubled, had he been better able to assimilate within the medical establishment, perhaps his name would today be spoken of by all surgeons. It was not to be.
As a medical student at Harvard, he and his best friend, Harvey Cushing, later to become a renowned neurosurgeon, developed what they termed “the ether record.” Now the standard anaesthesiology record kept on every case, noting vital signs and the types and amounts of agents given, Codman and Cushing used it to see if they could improve their own ability at giving ether. As students on the anesthesiology rotation their first two cases had died, and they sought a better way.6,8,9
When Codman began his practice in Boston in 1895, his first official title was “skiagrapher” to the Boston Children’s Hospital. Skiagraphy was the original term for radiology (skia = shadow in Greek), and Codman became fascinated with the new modality for diagnosing illness and injury. He produced the first atlas of normal skeletal radiographs, which still exists and can be viewed at the Countway Library of the Harvard Medical School. He wrote several articles in the early days of radiology, including the first published case of a scaphoid fracture diagnosed by x-ray.7 In those early days of ultra-high radiation doses, his research into x-rays has been postulated to have caused both his inability to father any children, and his ultimate demise from melanoma.
Codman settled into his practice of general surgery in the first decade of the 20th century. From 1900-1920, he became one of the busiest,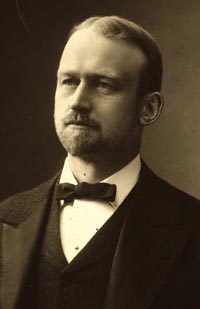 most accomplished, and most published surgeons at Mass General. By 1910, he had published over 30 papers on the study of duodenal ulcers and was the first practitioner to study this problem closely among general surgeons. Interestingly, Codman also suffered from the problem, and had surgery on it in England while there at a meeting. It is not known if his affliction stirred his interest in the topic.
most accomplished, and most published surgeons at Mass General. By 1910, he had published over 30 papers on the study of duodenal ulcers and was the first practitioner to study this problem closely among general surgeons. Interestingly, Codman also suffered from the problem, and had surgery on it in England while there at a meeting. It is not known if his affliction stirred his interest in the topic.
To most orthopaedists who know of Codman, if they do at all, he is usually considered important for two other fields – shoulder surgery and bone sarcoma. In both fields, Codman is considered the pioneer. In shoulder surgery, Codman is usually considered with Charles Neer as the two beacons that have illuminated the field. Codman developed his interest in the shoulder while studying as a medical student in the 1890s in Germany. There he saw several operations on the rotator cuff and sub-acromial bursa, and spent time in the anatomy lab dissecting the shoulder.7
In 1911 and 1912, Codman published the first two known cases (in English) of repair of a rotator cuff tear. Throughout his career he continued his study of the shoulder, which culminated in 1934 with the publication of his life’s great work, The Shoulder: Rupture of the Supraspinatus Tendon and Other Lesions In or About the Subacromial Bursa, which was the first book ever written solely on the shoulder in English. The book is still pertinent today and should be studied by any practicing shoulder surgeon. It begins with an autobiographical preface, and ends with a similar autobiographical epilogue. In between one finds over 400 pages of shoulder wisdom.5 It was decades ahead of its time. Codman described the pathology of rotator cuff disease, shoulder anatomy and biomechanics, shoulder rehabilitation, a classification of proximal humeral fractures, neurologic disorders about the shoulder, and tumors about the shoulder. He only briefly mentions instability, and shoulder arthroplasty was not yet a reality, as it awaited the genius of Neer to make that a reality.
This was Codman’s second book that could be considered more than a small monograph. He had published the first in 1925. Entitled simply Bone Sarcoma, it was the result of five years of study of the topic. His interest began when a close friend was diagnosed with a bone tumor and Codman’s research led to his formation of the Registry of Bone Sarcoma, which was the first cancer registry in the United States. During his work on bone sarcoma, Codman described the triangular periosteal elevation of osteosarcoma, now known as Codman’s triangle, although he actually described it in a case of Ewing’s sarcoma. He also described what he termed “chondromatous epiphyseal giant cell tumors of the [proximal] humerus,” a tumor we now know as a chondroblastoma, often called Codman’s tumor. For his work on bone sarcoma, shortly before his own death, Codman was given a gold medal by the AAOS.4 Codman’s slides for the Registry of Bone Sarcoma still survive and are housed at the Armed Forces Institute of Pathology (AFIP)
.
The Registry of Bone Sarcoma was typical Codman. It was an attempt to look at a problem in detail and see how it could be solved, what could be done better. He had begun such study around 1905, when he began to look at the problem of outcomes. To Codman, he called these “End Results” and he considered this the “End Result Idea.” He knew it was revolutionary, but he continually challenged physicians to study and document their own End Results. He defined the idea simply:
The common sense notion that every hospital should follow every patient it treats, long enough to determine whether or not the treatment has been successful, and then to inquire, “If not, why not?” with a view to preventing similar failures in the future.5
Common sense it may have seemed, but it was simply not done. Codman was not only the first orthopaedist to suggest that we should study outcomes, he was the first physician to do so. Prior to him, only Florence Nightingale had promulgated the idea. To them, we owe the genesis of outcome studies and evidence-based medicine.1,6,7,8,9
Codman kept track of his patients via “End Result Cards.” Basically index cards, they contained some basic demographic data on every patient he treated, along with the diagnosis, the treatment he rendered, and the outcome of each case. He followed up every patient for at least one year to obtain long-term outcomes. Unfortunately the End Result Cards have not survived. Through 1910 Codman wrote several papers on the End Result Idea. There was little response from local surgeons, but nationally there was some curiosity, mostly from Edward Martin, a Philadelphia gynecologist. He and Codman helped start the American College of Surgeons (ACS) in 1910. Together they formed several committees of the ACS, one chaired by Codman – the Committee for Hospital Standardization.7
The Committee for Hospital Standardization began as an attempt to study hospital outcomes (end results) and see how they could be improved. Codman wrote, “We believe it is the duty of every hospital to establish a follow-up system, so that as far as possible the result of every case will be available at all times for investigation by members of the staff, the trustees, or administration, or by other authorized investigators or statisticians.”7
 Originally, the Committee asked that hospitals meet five simple guidelines – 1) each hospital should have a medical staff, 2) the members of the medical staff should be chosen based on graduation from medical school (not a given in that era), competency, and character, 3) there should be regular staff meetings to review cases (end results – in this case the forerunner of morbidity and mortality conferences), 4) medical records should be written and filed for all cases, and 5) each hospital should have a clinical laboratory and radiology section. It should be noted that, when this was written, no medical records at all were produced for many patients. The patients were admitted, treated, and all the care was kept inside the physicians’ head.
Originally, the Committee asked that hospitals meet five simple guidelines – 1) each hospital should have a medical staff, 2) the members of the medical staff should be chosen based on graduation from medical school (not a given in that era), competency, and character, 3) there should be regular staff meetings to review cases (end results – in this case the forerunner of morbidity and mortality conferences), 4) medical records should be written and filed for all cases, and 5) each hospital should have a clinical laboratory and radiology section. It should be noted that, when this was written, no medical records at all were produced for many patients. The patients were admitted, treated, and all the care was kept inside the physicians’ head.
Though these guidelines now seem risible, when the first trials of the ACS were produced, only 89 of 692 hospitals passed. The results were announced at the Waldorf Astoria in New York, and the papers were burned after the meeting so that the public could not know which hospitals had failed. The Committee still exists today, but over the passage of years has transmogrified into the Joint Commission for Accreditation of Hospital Organizations (JCAHO).7,8,9
As Codman was starting what would become the JCAHO, he resigned in a controversial protest from Mass General and opened his own hospital. Codman’s protest was that Mass General would not implement the End Result Idea and force their physicians to publish their outcomes. His hospital was called the Codman Hospital, and unlike the hospital he left, he required all staff members, which briefly included Harvey Cushing, to study and publish their own end results. Codman himself wrote three small pamphlets, all with the main title of A Study in Hospital Efficiency. In these pamphlets, he published the results of every case he took care of at the Codman Hospital, using his End Result Cards for background data. Stunning in their honesty, the reports would never be attempted today due to the fear of litigation. He classified his complications under such headings as “Errors Due to Lack of Judgment,” and “Errors Due to Lack of Technical Skill.”3
But still few doctors heard him. On 6 January 1915, Codman chaired the meeting of the Suffolk District Surgical Society (Boston is in Suffolk County). He listened to several other speakers, all experts in the field of hospital administration, including the mayor of Boston, James Curley, who was known for his support of public health initiatives. Codman then stood to speak and unveiled a cartoon he had drawn. It showed an ostrich with its head in the sand, kicking up sand behind him, all the while digging up golden eggs. Codman explained that the ostrich typified surgeons and hospital administrators, who had their heads in the sand, never studied their own End Results, but were content as long as they produced the “golden eggs.”1,5,6,7,8,9
including the mayor of Boston, James Curley, who was known for his support of public health initiatives. Codman then stood to speak and unveiled a cartoon he had drawn. It showed an ostrich with its head in the sand, kicking up sand behind him, all the while digging up golden eggs. Codman explained that the ostrich typified surgeons and hospital administrators, who had their heads in the sand, never studied their own End Results, but were content as long as they produced the “golden eggs.”1,5,6,7,8,9
It was not well-received. Several doctors got up and left in a huff. Others accosted him verbally and tempers had to be calmed. Codman was asked to resign as chairman of the Surgical Society and his practice suffered. External events would later add to the damage.
On 5 December 1917, two munition ships, the Imo and the Mont Blanc, refueled in Halifax Harbour in Nova Scotia, anchoring near there overnite. The next morning, at 9 AM, they collided in the harbour, with the result being the largest man-made explosion in the history of the world, until the advent of World War II and the atomic bomb. Over 3,000 people were killed in a city of 60,000 people, and many more were blinded by the remnants of the explosion and flying glass. Codman had many friends in Nova Scotia, a place he had visited many times for hunting and fishing trips. The day after the explosion he took a train from Boston, along with some of the nurses from the Codman Hospital, and set up a mobile hospital in Halifax, staying there for over two weeks to treat the survivors of the explosion.
World War I was soon upon the United States, and when Codman returned from Halifax, he enlisted in the Army. He was stationed mostly at Camp Taylor, Kentucky. While he did not see overseas duty, his work in the Army was harrowing because of the 1918 influenza pandemic, considered the greatest pandemic in the history of mankind. Possibly as many as 50 million people died world-wide from influenza, and its precise cause is still being studied. It is postulated that it began among the American military and was spread world-wide when the US Army was mobilized to Europe. Codman’s wards were filled with flu-stricken troops, who were under his care. Codman soldiered on, working almost inhuman hours while caring for the dying. When Codman finished his tour of duty, he had little medical practice remaining. He had spent over a decade urging fellow physicians to study their own outcomes, their end results, all to no avail. He had alienated himself in the process, speaking up where others would not, claiming his results were better than all others, which was likely true, because only he could produce any outcomes. On his return to Boston, ostracized by his peers, out of mind now for almost two years, except to remember his obstreperous tirades against them, there were no referrals, there were few patients, and there was little income.7
Codman struggled on. In the 1920s, Harvard gave him a small room to work from, and he began the Registry of Bone Sarcoma, surviving on his wife’s family money.4 As he reached his 60s, there was little of that left, and his life was bereft of much else. He and his wife had no children. They lived with their several dogs, who always accompanied Codman on his many days on the lakes and in the woods, hunting or fishing. And they lived mostly apart, 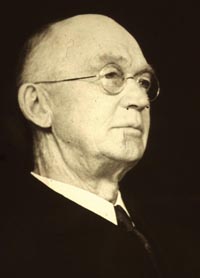 Codman at their country home in Ponkapoag (a part of Milton, just south of Boston), and his wife, Katherine, at their Boston brownstone.
Codman at their country home in Ponkapoag (a part of Milton, just south of Boston), and his wife, Katherine, at their Boston brownstone.
During his last months, he inquired about the cost of a headstone. It was seemingly more of a financial burden than he wished to leave his wife, as none was ever purchased. After dying from melanoma on 23 November 1940, he was interred in Cambridge at the Mount Auburn Cemetery. He lies in an unmarked grave in his wife’s family plot.7
He did not expect much from his colleagues, and he had predicted this years before. He once noted, “Honors, except those I have thrust upon myself, are conspicuously absent…, but I am able to enjoy the hypothesis that I may receive some more from a more receptive generation.”5 That generation may still await, but hopefully is now upon us.
Six fields of medicine. In three of them he was an important contributor, in two of them he was an absolute giant of the field, and in one he was a revolutionary who was so far ahead of his time that his accomplishments could not, or would not, be appreciated by his peers. Any doctor of the 20th century making the contributions which Codman made in one or two fields would be long remembered. But as Berwick noted, “Codman looked ahead. He looked, indeed, beyond us. Seventy-eight years ago he began his life’s work; forty-eight years ago he died. Are we ready for him yet?”7
In Amory Codman’s lifetime, no appreciation was given him. In fact, his efforts to reform medical science by starting the field of outcome studies brought him mostly ridicule, censure, and poverty. At his death, his newspaper obituaries mentioned only two of the six fields to which he contributed – bone sarcoma and shoulder surgery.7
The End Result Idea was never mentioned.
He was the best of us. 
References
1. Berwick D. M. "E. A. Codman and the rhetoric of battle: a commentary." Milbank Quarterly, 67(2): 262-267, 1989. 2. Codman, E. A. "Committee for Standardization of Hospitals [of the American College of Surgeons]. Minimum standard for hospitals." Bull Am Coll Surg, 8: 4, 1924.. 3. Codman E. A. A Study in Hospital Efficiency. As Demonstrated by the Case Report of the First Five Years of a Private Hospital. Boston: Thomas Todd Co., 1918-1920.. 4. Codman E. A. Bone Sarcoma: An Interpretation of the Nomenclature Used by the Committee on the Registry of Bone Sarcoma of the American College of Surgeons. New York: Paul B. Hoeber, Inc., 1925.. 5. Codman E. A. The Shoulder: Rupture of the Supraspinatus Tendon and Other Lesions In or About the Subacromial Bursa. Boston: Thomas Todd Co., 1934.. 6. Donabedian A. "The end results of health care: Ernest Codman's contribution to quality assessment and beyond. " Milbank Quarterly, 67(2): 233-256, 1989.. 7. Mallon, Bill. Ernest Amory Codman: The End Result of a Life in Medicine. Philadelphia: W. B. Saunders, 1999.. 8. Neuhauser D. "Ernest Amory Codman, M.D., and end results of medical care." Int J Tech Assessment Health Care, 6: 307-325, 1990.. 9. Reverby S. "Stealing the golden eggs: Ernest Amory Codman and the science and management of medicine." Bull History Med, 55: 156-171, 1981..